
Neurosurgeon – Sydney | Tamworth
Dr Gordon Dandie – MBBS, FRACS
Dr Gordon Dandie
Neurosurgeon | Spine Surgeon

![]()
Dr Gordon Dandie is a highly qualified and experienced Neurosurgeon and Spine Surgeon.
.
He is extensively trained in the management and treatment of complex spine conditions, brain tumours and cerebrovascular lesions, with a strong focus on minimally invasive surgical techniques and Robotic Assisted Surgery.
.
Dr Dandie is a Visiting Medical Officer at Westmead Private Hospital and Sydney Adventist Hospital.
Dr Gordon Dandie:
“I aim to provide a calm, focused and supportive environment for all of my patients. I take special care and time to explain all aspects of my patients medical findings and work hard to ensure they feel comfortable with the available treatment options.”
— About Dr Gordon Dandie —
Neurosurgeon & Spine Surgeon – MBBS, FRACS.
Dr Gordon Dandie specialises in complex spinal surgery, neurovascular surgery, and brain tumour surgery. He has particular expertise in minimally invasive (keyhole) surgery and robotic assisted surgery.
Dr Dandie was the first surgeon in the southern hemisphere to use the ROSA robotic system for spinal surgery.
.
Find out more about Dr Dandie’s professional medical education, training, skills and experience:
— Education —
Completed Bachelor of Medicine and Bachelor of Surgery (MBBS) at the University of New South Wales 1985-1989.

————————-
Internship and Basic Surgical Training undertaken at St Vincent’s Hospital, Sydney 1990-1992.

————————-
Completed basic neurosurgical training at St Vincent’s Hospital and Royal Hobart Hospital 1993-1995.
— Specialist Training —
Advanced neurosurgical training undertaken at St Vincent’s Hospital, Royal North Shore Hospital, and the Sydney Children’s Hospital Randwick 1996-1999.
Dr Dandie obtained his FRACS qualification in 2000.
![]()
FRACS stands for Fellow of the Royal Australasian College of Surgeons.
This qualification is only awarded to specialist surgeons who have completed a minimum of 12 years medical and surgical education, with at least 5 years of specialist postgraduate training.
.— Post Fellowship Training —
Cerebrovascular (Aneurysm/AVM) Training
Royal North Shore Hospital – 2000
————————-
Complex Spinal Surgery Fellowship
University of Toronto, Ontario, Canada – 2001.

.
.— Specialist Appointments —
Dr Dandie works as a Visiting Medical Officer (VMO) at:
Westmead Private Hospital
Sydney Adventist Hospital (The San)
————————-
He is Head of Department of Neurosurgery and a member of the Medical Advisory Committee at Westmead Private Hospital.

————————-
Past Secretary of the NSW Neurosurgical Association, and a Board member of the Sydney Neuro Oncology Group, 2007 – 2017.
————————-
Became an accredited medical officer at Sydney Adventist Hospital, 2007.

— Teaching Appointments —
Clinical Senior Lecturer University of Sydney.
![]()
Dr Dandie is extensively involved in teaching trainees and surgeons nationally and internationally.
— Professional Memberships —
![]()
Spine Society of Australia.
![]()
Australian Medical Association.
![]()
Neurosurgical Society of Australasia.
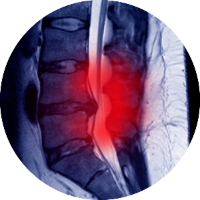
— Spine Surgery —

“Dr Dandie has extensive experience in spine surgery and understands the pain and confronting issues associated with a spinal problems.
He will compassionately, thoroughly and expertly explain and guide you through the process and the options available to you.”
Traditional Spine Surgery Verses Minimally Invasive Spine Surgery
Traditional spine surgery – Called “open surgery” involves a long incision that cuts through the skin, muscle and soft tissue around the area to allow the surgeon to view and access the spine. This causes significant trauma to the muscle and surrounding areas that can lead to a lengthier recovery period and may also increase both blood loss and the risk of infection.
Minimally invasive spine surgery – Doctors use specialised instruments to access the spine through small incisions and split rather than cut the underlying muscle. This avoids significant damage to the muscles surrounding the spine. Typically, this results in less pain after surgery, less bleeding, and shorter stays in the hospital and a faster recovery.
Where applicable Dr Dandie will use minimally invasive spine surgery.
Microdiscectomy
Microdiscectomy is used to treat symptoms of sciatica (nerve pain) due to a lumbar disc herniation. The goal of microdiscectomy surgery is to relieve pressure on the nerve.
A microdiscectomy is performed under general anaesthetic with a small incision, 2 to 3 cm long, made in the lower part of the back in the midline, at the level where the disc prolapse has occurred.
During the procedure, the herniated (detached) disc material under the nerve root is taken out with the aid of a microscope.
The removal of the pressure on the nerve may immediately improve the associated leg pain symptoms.
Artificial Disc Replacement
Artificial disc replacement surgery involves replacing a damaged, painful or herniated disc with an artificial disc.
The surgery may be performed on the lower back (lumbar spine) or the neck (cervical spine) and is recommended when nonsurgical treatments have been exhausted and the associated pain without treatment is significantly affecting your quality of life.
The artificial discs are designed with the goal of mimicking the form and function of the spine’s natural disc.

Laminectomy
A laminectomy is a surgical procedure that removes the back part of the vertebra that covers your spinal canal (called the lamina).
The aim of laminectomy is to enlarge your spinal canal to relieve pressure on the spinal cord or nerves, commonly caused by bony spur, arthritis or bulging disc within the spinal canal.
Increased pressure on your spinal cord may cause nerve pain, numbness and/or weakness in your arms, hands or legs.
Laminectomy is generally used only when more-conservative treatments such as physical therapy, medication or injections have failed to relieve symptoms.

Spinal Fusion
Spinal fusion is surgery to join two or more vertebrae into one single structure. The goal is to stop movement between the two bones and prevent instability and pain. Once they’re fused, they no longer move like they used to. This prevents nerve compression and joint inflamation that may have caused discomfort.
To fuse the vertebrae together permanently, the surgeon places the bone graft material between the vertebrae. Metal plates, screws or rods may be used to help hold the vertebrae together while the bone graft heals.
Minimally Invasive Spinal Surgery (MISS) techniques have completely changed how spinal fusion operations are performed and have improved patient outcomes significantly.

Spinal deformity correction
Spinal deformity refers to conditions where the spine is out of balance or the vertebra are out of alignment relative to one another. Spinal imbalance often involves long segments of the spine.
As we age the intervertebral discs dehydrate and lose height. This has the effect of tilting our spinal column forward and our muscles have to work harder to maintain posture which may lead to chronic spinal pain.
Spinal deformity can also cause compression of the spinal cord causing pain or neurological dysfunction.

SPONDYLOLISTHESIS is a spinal deformity where one vertebrae slips forward relative to the one below. This is most common in the lumbar region and can be due to many causes including congenital, trauma, degenerative disease or previous surgery. This can also cause chronic spinal pain and nerve compression resulting in leg pain.
Surgical advancements have led to muscle sparing techniques that have made spinal operations less invasive and much easier for the surgeon and patient.
— Neurosurgery —

Dr Dandie has extensive neurosurgery experience and understands the anxiety and physical difficulties associated with Intracranial conditions.
He will compassionately, thoroughly and expertly explain and guide you through the process and options available.
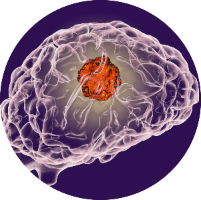
Brain Tumour
A brain tumour may be inside your brain or next to your brain and push on the brain’s surface. Tumours may grow and press harmfully against healthy brain tissue and cause headaches, seizures, visual problems or weakness in your arms and legs.
Other brain tumours may cause no symptoms and may be diagnosed during investigations ordered for other reasons. The diagnosis of a brain tumour generally requires a scan of the brain, usually a CT or MRI.
The options for treating brain tumours include surgery to remove the tumour, surgical biopsy, or adopting a watch-and-wait approach. Sometimes treatment with radiotherapy and chemotherapy will be recommended.
I understand how confronting a positive diagnosis can be for you and your family. I will take the time to ensure you understand the non-surgical and surgical management options, risks, hospital stay information, wound care, activity guidelines and follow up appointments to assess and monitor your progress.
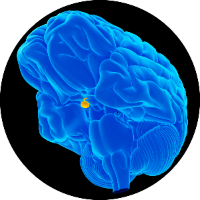
Pituitary Tumour
The pituitary gland is a pea-sized structure located at the base of the brain just behind the nose. It oversees the other glands of the endocrine system and controls hormone levels throughout the body.
A pituitary tumour (also called an adenoma) is a mass of cells that grow on the gland that may bring about a change in hormone production somewhere else in the system by releasing its own ‘stimulating’ hormones.
Some pituitary adenomas don’t produce excess hormones but may enlarge and cause pressure on the eye nerves leading to gradual loss of vision.
Generally, pituitary tumours are benign (not cancerous) and slow growing, and pituitary cancers are rare. Benign tumours don’t spread to other parts of the body, so there is no chance of secondary tumours developing.
Many pituitary tumours don’t require treatment and can be observed with serial scans. If they are causing symptoms treatment may include surgery, radiation therapy and medication.
Cerebral Aneurysms
A cerebral aneurysm (or brain aneurysm) is a bulging, weak or thin spot on an artery in the brain that balloons out and fills with blood.
This results in an abnormal widening or ballooning of the vessel wall that may put pressure on the nearby nerves or brain tissue.
Brain aneurysms can burst, spilling blood into the surrounding tissue (called a hemorrhage) and can cause serious health problems such as hemorrhagic stroke, brain damage, coma, and even death.
As some aneurysms are life threatening it is important to be assessed by a trained cerebrovascular surgeon.

Vascular Malformations
Vascular malformations are abnormal collections of blood vessels in the brain tissue. Two of the more common malformations are:
- ARTERIOVENOUS MALFORMATIONS
- CAVERNOMAS.
They can occur anywhere in the brain and are usually congenital. The malformations can cause symptoms such as headache or seizures. As the blood vessels are not normal they have weak walls and can leak or bleed and cause a stroke.
Not all malformations need treatment but maybe observed. Other treatments may involve embolisation and/or radiotherapy. Microsurgical resection of the malformation is sometimes the safest and most effective treatment.
Trigeminal Neuralgia
The trigeminal nerve carries sensation from your face to your brain. If you have trigeminal neuralgia, even mild stimulation of your face such as brushing your teeth may trigger a jolt of excruciating pain.
Trigeminal neuralgia can progress from short mild attacks to longer, more-frequent bouts of searing pain.
There are a variety of treatment options available, so you’re not doomed to a life of pain.
Trigeminal neuralgia can usually be effectively managed with medications, injections or surgery.

— Appointments & fees —
What do you need
For your first appointment with Dr Dandie please:
- Arrive 10 minutes early to fill out any necessary paperwork
- Bring your referral from your specialist or GP
- Bring your Medicare card and Private Health Insurance details
- Copies of all X-rays and scan images relevant to your condition.

Dr Dandie will need to see the Xray and scan pictures at your consultation.
Please bring these pictures on film/CD/memory stick, as viewing the images online may not be possible during the consultation.
If your Xrays or scans were done at a public hospital you will need to collect copies from the hospital as these are not available online to Dr Dandie.
During your appointment
Initial appointments are 40 minutes – Dr Dandie will:
- Listen to the history of your condition and ask questions for clarification
- He will perform an examination of your neurological system
- Review your imaging, reports and test results.
He’ll then discuss your diagnosis, history of the condition and potential management options.
.
Dr Dandie aims to ensure you:
- Understand your condition
- Feel comfortable asking any questions
He’ll take the time to answer any questions you may have to help you make an informed decision about the management of your condition. In 9 out of 10 cases, treatment does not involve an operation.
After the consultation you will be provided with forms or referrals for further tests or treatments as required.
.
Follow-up appointments
Follow-up appointments are usually 20 minutes – Please bring:
- OLD X-rays, scans and reports and;
- NEW images and reports to your appointment.
If you have any further questions or concerns about your condition after your consultation, please write them down and book a follow-up appointment.
Fee information
For fee information, please call Kate or Laura on (02) 8123 0140.
You can conveniently fix up your account at the time of consultation by cash or credit card.
![]()



Surgical fees
In most circumstances Dr Dandie does not charge a gap fee, meaning his surgical fees will be fully covered by the patient’s private medical insurance.
NIB Insured Patients – Patients insured with NIB will be charged a gap in the event of having an operation, as the “No Gap” payments this insurer provides to surgeons and anaesthetists are significantly below the industry average.
— Contact Dr Gordon Dandie —
If you have any questions, please do not hesitate to contact my practice rooms:

Dr Gordon Dandie
Neurosurgeon – MBBS, FRACS.
![]()
For all enquiries and appointments:
(02) 8123 0140
admin@dandieneurosurgical.com.au
(02) 9633 9789

Meet the team at Dandie Neurosurgical – Kate, Dr Dandie and Laura.
Practice Locations
Dr Dandie consults in three locations, two in Sydney and one in Tamworth:
PARKWAY SAN CLINIC
Suite 210
172 Fox Valley Road
…… Wahroonga NSW 2076.
(02) 8123 0140
(02) 9633 9789
Disabled parking and wheelchair access.
WESTMEAD PRIVATE HOSPITAL
Suite 203
Corner Mons and Darcy Roads
…… Westmead, Sydney, NSW 2145.
(02) 8123 0140
(02) 9633 9789
Disabled parking and wheelchair access.
NORTHWEST NEUROLOGY
96 Marius Street
Tamworth NSW 2340.
(02) 8123 0140
(02) 9633 9789
Disabled parking and wheelchair access.